You Are What You Eat
I, like most people, do not have the world’s best eating habits. I think in part that is because it is very hard to make food for one person. There are plenty of cookbooks for two people but not nearly enough for one. In addition, it is hard to make something and realize that you are going to spend all week eating the same food. And of course, with all this you also have to determine what is healthy enough to eat. Relying on food nutrition labels will only give you a so-so understanding of what you are consuming.
Nutrition Labels
I think that most people can probably agree that our current nutrition labels are less than helpful. Portion sizes on these tend to not reflect the way most people consume. Who really eats only 3 Oreos in a sitting? And not only are the portions misleading, but nutrition labels often contain a lot of confusing, scientific terms and leave you wondering what you are truly consuming, how good it is for you, and how much you should actually be consuming (possibly none). Earlier this year, the FDA proposed a new nutrition label that, in theory, is more in line with American eating habits.
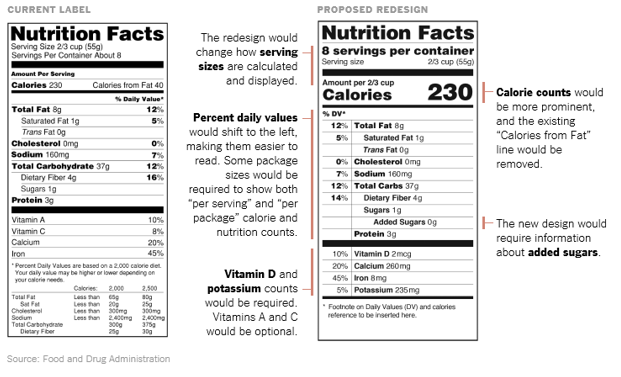
However, nutrition labels still hide a lot of information about food. According to Dr. David Kessler, the commissioner of the FDA, “although the numbers can look good, the product may not be real food and have no nutritional value.” But, at the very least the revisions require companies to list out the different types of sugar and provides a more accurate portion sized based on America’s eating habits.
One key challenge is that the measurements used are often hard to reconcile. You might be shocked to learn that a 20 ounce coke has 16 teaspoons of sugar. Eating pancakes for breakfast involves less sugar than that. In addition, since ingredients are listed separately it is hard to determine what is naturally in the product versus what was added during the processing of your food.
Juices are one of the worst offenders because most claim to be 100% juice but for many filtered water is listed as the main ingredient. Can something be 100% juice if you first ingredient is water?
Don’t Leave it All to the Label
For all of us who wish to know what we are consuming and how healthy the item is there is now a great resource. Environmental Working Group built a Food Score database. The site contains information on more than 80,000 items sold in groceries stores. The site offers details of ingredients, nutritional information, and how processed the food items are.

The site assigns food products a score from 1 to 10, with 1 being the best. The score is based on how nutritious it is, how many ingredients are in it, and an estimated how processed it is. The rating also includes information about whether the food product is organic, how the animals were raised, whether antibiotics were used, and if the food was exposed to dangerous environmental factors like pesticides. The site also tells you if it gluten-free, whether it potentially contains genetically modified ingredients, and how it stacks up to the competition. While the site isn’t perfect, it’s a great place to look if you want to better understand what you’re eating.
The Food Score database has also done broad analysis of trends found in different foods. They found that 60% of the products on the database contain added sugar. Shockingly, 90% of granola bars contain added sugar while 100% of stuffing mixes contain added sugar. And processed meats such as bologna and salami also contain added sugar.
Eating Right is Hard, But Worth it
Eating well is hard. The best choice is obviously to cook your own meals with foods that you have meticulously researched. Unfortunately, it is often hard to find the motivation and time to do so. But the new nutrition labels are a start, and for those who want to look deeper sites like the Food Database make it easier for us to make healthy choices. While finding and choosing the healthy option is sometimes inconvenient, it’s a smart choice.













